Primary Health Care (PHC.)
Primary Health Care is essential health caremade universally accessible to individuals and families
in the community by means acceptable to them,
through their full participation and at a cost that the
community and country can afford.
It forms an integral part both of the country's health system
of which it is the nucleus and of the overall social
and economic development of the community.
(WHR 2008)
การสาธารณสุขมูลฐาน (สสม.)
คือการสาธารณสุขที่เป็นความจำเป็นจะต้องมี การสาธารณสุขที่เป็นงานหลัก (essential health care)จัดสร้างขึ้นเพื่อให้ทุกคนเข้าถึงได้ (made universally accessible)
ทั้งแต่ละบุคคลและครอบครัว (individuals and families)
โดยทีชุมชนมีส่วนร่วมอย่างเต็มที่ full participation)
โดยมีค่าใช้จ่ายที่ชุมชนและประเทศ สามารถจ่ายได้ (cost that the community and country can afford)
เชื่อมโยงกับระบบสาธารณสุขของประเทศ (the country's health system)
เป็นแกนกลางของการพัฒนาสังคมและเศรษฐกิจของชุมชน (social and economics development of the community)
(WHR 2008)
(Essential = เป็นสิ่งที่จำเป็นที่จะต้องมี เช่น Essential Drugs = บัญชียาหลัก)
Primary Health Care
ประเทศไทยมี อสม. 800,000 คน ซึ่งประเทศอื่นไม่มี *งานในปี 2007-2008 ที่ อสม. ของไทยทำได้ผลดึก็คือ การควบคุมไข้หวัดนกในสัตว์ปีก
แก้ข่าวร้าย กระจายข่าวดี ชี้บริการ ประสานงานสาธารณสุข
บำบัดทุกข์ประชาชน ทำตนเป็นตัวอย่างที่ดี
เปลี่ยน สถานีอนามัย เป็น PCU มีแพทย์ หรือ มี พยาบาล เพิ่มเติม อาจเต็มเวลา หรือ Part time
ทำไม PHC ในไทยจึงต่างกับต่างประเทศ
เพราะประเทศอื่นอาจมี บุคลากร งบประมาณ การจัดการด้านสาธารณสุขดีกว่าพร้อมกว่าประเทศไทยจึงเลือกวิธีจัดให้มี ผสส/อสม และต่อมาเปลี่ยน ผสส ให้เป็น อสม.
World Health Report 2008
Primary Health Care (PHC) Now More Than Everwww.who.int/topics/primary_health_care/en/
PHC REFORMS
1. UNIVERSAL COVERAGE = to improve health equity, ...2. SERVICE DELIVERY =to make health systems people-centred, Reorganized Health Services as Primary Care, ...
3. LEADERSHIP = to make health authorities more reliable, ...
4. PUBLIC POLICY = to promote and protect the health of communities , ...
|
UNIVERSAL COVERAGE REFORMS
to improve health equity ความเท่าเทียมกันด้านสุขภาพ |
SERVICE DELIVERY REFORMS
to make health systems people-centred Reorganized Health Services as Primary Care while producing better outcomes สร้างบริการสาธารณสุข (Health services)
LEADERSHIP REFORMS
| to make health authorities more reliable command and control on one hand and laissez-faire disengagement of the state on the other. ทางหนึ่ง คือควบคุมและกำกับ (command and control)
PUBLIC POLICY REFORMS
| integrating public health actions with primary care to promote and protect the health of communities persuing healthy public policys across sector บูรณาการงานด้านสาธารณสุขเข้ากับ Primary Care
|

|
http://www.who.int/whr/2008/en/index.html จะเกิดอันตรายถ้าหาก Primary Care แบบที่ใช้อยู่ในประเทศที่มีทรัพยากรมากพอ
|
| 1.
Primary Care เป็นสถานที่ ที่ผู้คนสามารถนำปัญหาสุขภาพในวงกว้างมาปรึกษาโรค
และไม่อาจยอมรับได้หากว่าในประเทศรายได้น้อยให้การดูแลเฉพาะโรคที่เลือกว่าเป็นเรื่องสำคัญเพียงไม่กี่โรค |
| 2.
Primary Care เป็นจุดเชื่อมต่อ (Hub) กับระบบสาธารณสุข (Health system)
และไม่อาจยอมรับได้ หากว่าในประเทศรายได้น้อย Primary Care ทำงานเพียงแต่แนะนำให้ผู้ป่วยไปเข้าระบบสาธารณสุข (guided through the health system), Primary Care ถูกจัดให้ลดระดับลงเป็นสถานีอนามัย (Health Post) ที่ทำงานตามลำพัง (Standalone) หรือเจ้าหน้าที่สาธารณสุขชุมชนที่แยกส่วนออกไป (Isolated Community Health Worker) |
| 3.
ความสัมพันธ์ระหว่างคนไข้กับบุคลากรการแพทย์ (Clinicians ongoing relationships)
ประชาชนมีส่วนร่วมในการตัดสินใจในเรื่องสุขภาพของตัวเขาเองและเรืองการสาธารณสุข (decision-making about their health and health care) เป็นสะพานเชื่อมต่อระหว่างบุคลากรสาธารณสุข และผู้ป่วย (it builds bridges between personal health care and patients) ในประเทศรายได้น้อยการจัดลำดับความสำคัญของปัญหาสาธารณสุข อาจมีแค่ช่องทางเดียว |
| 4.
Primary Care เปิดให้มีโอกาส ส่งเสริมสุขภาพ (health promotion)
ป้องกันโรค (disease prevention ) และ ค้นหาโรคตั้งแต่เริ่มต้นป่วย (early detection) และไม่อาจยอมรับได้ ถ้าหากในประเทศที่รายได้น้อย มีแต่รักษาโรคอย่างเดียว |
| 5.
Primary Care ต้องมีทีมแต่ละสาขาวิชาขีพ (Teams of health professionals) :
แพทย์ (Physicians), พยาบาลเวชปฎิบัติ (Nurse Practitioners), และผู้ช่วย (Assistances) ซึ่งมีความสามารถเฉพาะเรื่อง ฺ(Specific) และเชี่ยวชาญด้านชีวการแพทย์และสังคม (Sophisticated Biomedical and Social Skills) และไม่อาจยอมรับได้ถ้าหากในประเทศยากจนมีแต่ผู้ดูแลประเภท non-professional ที่ไม่ใช่ แพทย์, พยาบาลเวชปฎิบัติ และผู้ช่วย |
| 6.
Primary Care ต้องการการจัดสรรทรัพยากรที่ควรต้องมี (Adequate resources) และการลงทุน (Invesment)
และไม่อาจยอมรับได้ถ้าหากในประเทศยากจนประชาชนต้องจ่ายเงินเอง (Out of pocket payment) โดยที่คาดว่าประชาชนที่ยากจนเหล่านั้นคงจะสามารถจ่ายเองได้ |
(WHR 2008, Box 2. Page XVii)
What has been considered primary care in well-resourced contexts
|
|
Primary care has been defined, described and studied extensively in well-resourced contexts, often with reference to
physicians with a specialization in family medicine or general practice. These descriptions provide a far more ambitious agenda than the unacceptably restrictive and off-putting primary-care recipes that have been touted for low-income countries |
| 1.
primary care provides a place to which people can bring a wide range of health problems
it is not acceptable that in low-income countries primary care would only deal with a few priority diseases; |
| 2. primary care is a hub from which patients are guided through the health system
it is not acceptable that, in low-income countries, primary care would be reduced to a stand-alone health post or isolated community-health worker; |
| 3.
primary care facilitates ongoing relationships between patients and clinicians, within which patients participate in decision-making about their health and health care; it builds bridges between personal health care and patients families and communities it is not acceptable that, in low-income countries, primary care would be restricted to a one-way delivery channel for priority health interventions; |
| 4.
primary care opens opportunities for disease prevention and health promotion as well as early detection of disease
it is not acceptable that, in low-income countries, primary care would just be about treating common ailments; |
| 5.
primary care requires teams of health professionals: physicians, nurse practitioners, and assistants with specific and sophisticated biomedical and social skills it is not acceptable that, in low-income countries, primary care would be synonymous with low-tech, non-professional care for the rural poor who cannot afford any better; |
| 6.
primary care requires adequate resources and investment, and can then provide much better value for money than its alternatives it is not acceptable that, in low-income countries, primary care would have to be financed through out-of-pocket payments on the erroneous assumption that it is cheap and the poor should be able to afford it. |
Primary Cares Key Attributes
(Starfield: 1998)
First contactLongitudinality (Patient focused over-time)
Comprehensiveness
Coordination (Information and Care)
First Contact บุคคล (และสถานที่) ได้พบกับคนใข้เป็นจุดแรก
Longitudinality ดูแลต่อเนื่องไปตลอด (ถ้าส่งไปที่อื่นรักษาทุเลาแล้วให้ส่งกลับมาดูแลต่อ)
Comprehensiveness ส่งเสริมสุขภาพ ป้องกันโรค รักษา ฟื้นฟู
Coordination การร่วมมือกัน ถ้าเป็นโรคที่ยาก โรคที่ซับซ้อน ส่งต่อไปรักษา ส่งต่อข้อมูล
Blog KM. Prof. Vicharn Panich
คุณหมอสมศักดิ์ ชุณหรัศมิ์ หัวหน้าทีมศึกษาสถานภาพของระบบบริการสุขภาพปฐมภูมิในประเทศไทยได้ให้นิยามของรับบบริการสุขภาพปฐมภูมิในบริบทไทย ไว้ดังนี้
เครือข่ายบริการสุขภาพที่ประกอบด้วย สถานพยาบาลที่มีแพทย์เวชปฏิบัติทั่วไป หรือแพทย์เวชศาสตร์ครอบครัว ประจำในการให้บริการ
เช่น โรงพยาบาลชุมชนขนาดเล็ก หรือศูนย์แพทย์ชุมชน และมาสถานีอนามัย หรือหน่วยบริการขนาดเล็ก จำนวนหนึ่ง ที่มิได้มี
แพทย์ประจำ เป็นลูกข่ายในการให้บริการ โดยมีพื้นที่และจำนวนประชากรที่ต้องดูแล ชัดเจนกลุ่มหนึ่ง เช่น ๑๐,๐๐๐ ๑๕,๐๐๐ คน
และมีการสนับสนุนเชื่อมโยงกัน โดยอาศัยระบบข้อมูล การส่งต่อ และการสนับสนุนด้านความรู้และทรัพยากร
http://gotoknow.org/blog/thaikm/219232
13 ตค.2551
Health System
Health System = Health Care + Health Services + ...Medical Care อยู่ใน Health Care เพราะคำว่า Health กว้างกว่า Medical
คือมีกระทรวงสาธารณสุข Ministry of Public Health (MoPH)
ซึ่งดูแล โรงพยาบาลของกรมการแพทย์ รพ.ของกรมควบคุมโรค
และ รพศ/รพท/รพชและสอ. สำนักงานปลัดกระทรวงสาธารณสุข
EQESA (Equity, Quality, Efficiency, Social Accountability)
Equity เท่าเทียม ตาม Health Need (ไม่ใช่ Demand)Equity เท่าเทียมกัน คือ คนตัวใหญ่เสื้อเบอร์ L, ปานกลาง เสื้อเบอร์ M, คนตัวเล็ก เสื้อเบอร์ S
Equity แบ่งได้เป็น Vertical ได้ตามร้อยละของเงินเดือน และ Horizontal ทุกคนได้เท่ากัน
Equality ได้เท่ากัน คือ One size fit all ทุกคนได้เสื้อเบอร์เดียวกัน
Quality = Technical, Functional (Holistic, Integrated, Continuous)
Efficiency = โรคที่รักษาได้ป้องกันได้ จัดการที่ Primary Care หรือ FLHS
โรคซับซ้อนส่งต่อ รพศ/รพท โดยที่ไม่มีหลายขั้นตอนเกินไป
ควรมีเพียง 2 tiers คือ Primary care, Secondary care
(หลายขั้นตอนเกินไป เช่น จาก (1) อสม ส่งต่อไปที่ (2) สอ --> (3) สอ.เครือข่ายหัวหน้าโซน--> (4) PCU อำเภอเมือง --> (5) แพทย์ Specialist ที่ Secondary Care.
Social Accountability ความโปร่งใส ตรวจสอบได้
Health Care Reform Project (HCRP)
เนื่องจาก Health Care ยังไม่ดีนัก จึงต้อง Reform อย่างน้อย 4 ด้าน คืิอ1. Primary Care
2. Financial
3. Hospital Management
4. Advocacy (support Primary Care)
Medical Care
Primary Care เช่น PCUSecondary Care เช่น โรงพยาบาลชุมชน รพ.จังหวัด
Tertiary Care เช่น Regional Hospital (รพ.ศูนย์)
Super Tertiary เช่น Excellence Center = รพ.มหาวิทยาลัย
รพศูนย์ หลายแห่งในประเทศไทยมีภารกิจเพิ่มขึ้นจากเดิม เช่น
อุบล โคราช ขอนแก่น ลำปาง พิษณุโลก อุตรดิตถ์ นครสวรรค์ ชลบุรี หาดใหญ่
มีภารกิจ การผลิตบุคลากรการแพทย์ เช่น แพทย์เฉพาะทาง แพทย์ประจำบ้าน นิสิตแพทย์ นิสิตพยาบาล
เช่นเดียวกันกับ ภารกิจของ รพ.มหาวิทยาลัย มีงานบริการ ในระดับ Excellence Center
เช่น ผ่าตัดโรคหัวใจ ผ่าตัดเปลี่ยนไต โรคมะเร็ง ผ่าตัดสมองและ Multiple Injury จากอุบัติเหตการจราจร
Health Services
Primary Care เช่น First Line Health Services (FLHS) ใน ประเทศเบลเยียม (.pdf)เป็น Private Practice มีแพทย์ประจำแต่เรียก Health Services
อ่านต่อ: https://somed1.tripod.com/gp/การมีส่วนร่วมชองชุมชน
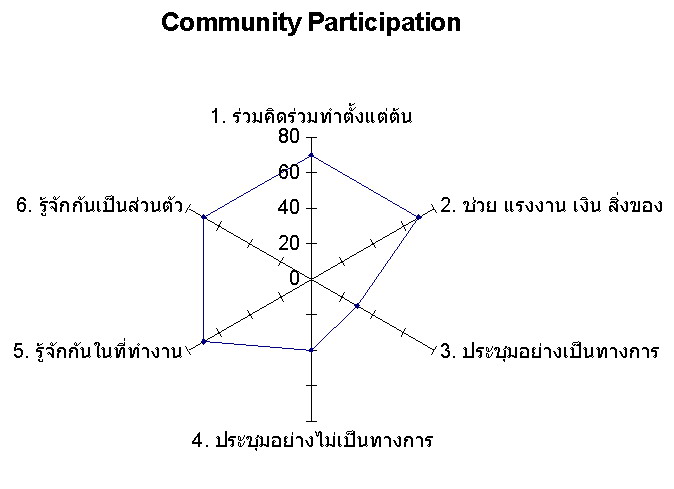
Community Participationเช่น ร่วมคิดร่วมทำตั้งแต่ต้น, ช่วย แรงงาน เงิน สิ่งของ
การประชุมเป็นทางการ, ไม่เป็นทางการ
การรู้จักกันในที่ทำงาน, การรู้จักกันเป็นส่วนตัว

[Back]